II. DESCRIPTION OF THE COMMUNITIES
A. History and Geography
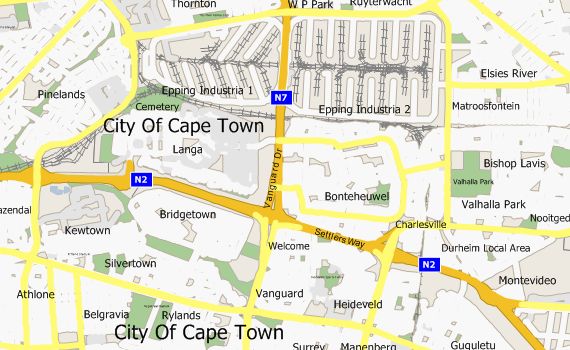
Figure 1. Map of Bonteheuwel and Langa
Bonteheuwel, originally Bonteheuwel Farm, was formed in 1965 as the Group Areas Act forced coloured people out of areas like District 6 and Diep River. Bonteheuwel is 352 hectares of land located 15 kilometers east of Cape Town. The community is divided into four sub-sections: Netreg, Golden Gate, Bonteheuwel and Kalksfontein.
Both Bonteheuwel and Langa are inconveniently located for access to employment, shopping and recreation. The Epping Industrial Area, which borders both townships to the north, is the only major source of nearby employment for residents of the communities.
Langa is a Xhosa word meaning sun. It was formed in 1927 as a result of the Urban Areas Act. Langa is named after a leader of the Hlubi people, Langalibalele, who was imprisoned in 1875 on Robben Island for resisting the local government in Natal. Langa is Cape Town’s oldest black African community and is located about 20 kilometers from the center of Cape Town. It is divided into two sections: Langa proper and the informal settlement, Joe Slovo. Langa is also adjacent to the suburb of Pinelands.
The N2 highway forms the southern border of Langa and Bonteheuwel, and Vanguard Drive runs between the two communities. Vanguard Community Health Centre is located on the Bonteheuwel side of Vanguard Drive. A footbridge connects the centre to Langa.
B. Demographics
According to the most recent census data, both Langa and Bonteheuwel are home to approximately 50,000 residents. However, these numbers are often in flux due to the transitory nature of many residents in the informal settlements. In Bonteheuwel, there are a higher percentage of females than males, which might be indicative of higher rates of gang violence and homicide among males in this community.
Table 1. Population Breakdown by Gender
Population by gender |
|||||||
Bonteheuwel |
Langa |
||||||
Male |
% |
Female |
% |
Male |
% |
Female |
% |
23988 |
47.3 |
26689 |
52.7 |
24448 |
49.2 |
25220 |
50.8 |
The populations in both communities are also very young, with almost fifty percent of the residents being under the age of twenty-five.
Table 2. Population Breakdown by Age
Population by age structure |
||||
Bonteheuwel |
Langa |
|||
Age |
Number |
% |
Number |
% |
0-24 yrs |
24486 |
48.3 |
24460 |
49.2 |
25-49 yrs |
17693 |
34.9 |
19955 |
39.2 |
50+ yrs |
8497 |
16.9 |
5250 |
10.6 |
*Statistics South Africa Census 2001 |
|
|||
C. Known Socioeconomic and Health Indicators
Although each community is home to roughly the same number of people, Bonteheuwel has greater physical resources than Langa. Bonteheuwel has about 5000 fewer housing units, but this reflects the prevalence of larger, more formal housing versus the high rates of informal shacks in Langa. Almost all Bonteheuwel residents have electricity and a solid majority has piped water, while in Langa only two-thirds have electricity and one-third water. Only nine percent of residents in Langa have a telephone versus almost half in Bonteheuwel.
Table 3. Socioeconomic Indicators
Socio-economic indicators |
||||
Bonteheuwel |
|
Langa |
||
Housing units |
10252 |
|
Housing units |
15514 |
Informal housing |
10% |
|
Informal housing |
47% |
Electricity |
99% |
|
Electricity |
66% |
Piped water |
84% |
|
Piped water |
35% |
Telephones |
47% |
|
Telephones |
9% |
Refuse removal weekly |
100% |
|
Refuse removal weekly |
92% |
|
|
|
|
|
*Statistics South Africa Census 2001 |
|
|
||
Both Langa and Bonteheuwel are troubled by unemployment. However, although similar percentages are employed in both communities, a higher percentage of residents are unemployed versus not economically active in Langa, while the opposite is true in Bonteheuwel. Also, the total number of residents represented in this table is less than the actual number of residents in the communities, suggesting questions about the accuracy of the data.
Table 4. Employment Statistics
Employment Statistics |
|||||||
Bonteheuwel |
|||||||
Employed |
% |
Unemployed |
% |
Not economically active |
% |
Total |
|
12929 |
39.8 |
7301 |
22.5 |
12264 |
37.7 |
32494 |
|
|
|
|
|
|
|
|
|
Langa |
|||||||
Employed |
% |
Unemployed |
% |
Not economically active |
% |
Total |
|
13127 |
36.2 |
12752 |
35.2 |
10361 |
28.6 |
36240 |
|
|
|
|
|
|
|
|
|
*Statistics South Africa Census 2001 |
|
|
|
|
|||
Data taken for both communities at the Vanguard Community Health Centre shows an increase in immunizations by almost fifteen percent. It also suggests increases in both the teen pregnancy and infant mortality rates. However, data from two separate clinics in Langa and Bonteheuwel suggests that teen pregnancy has gone down in both communities, while infant mortality has decreased in Langa and increased in Bonteheuwel.
Table 5. Health Indicators, Vanguard
Vanguard Community Health Centre |
||
Health indicators |
||
Infant Mortality rate |
2001/02 |
2002/03 |
(per 1000 live births) |
24.7 |
30.95 |
Teen Pregnancy rate |
6.2% |
7.3% |
Immunization rate |
84.4% |
98.7% |
Table 6. Health Indicators, Langa
Langa Clinic |
||
Health indicators |
||
Infant Mortality rate |
2001 |
2002 |
(per 1000 live births) |
30.9 |
20.3 |
Teen Pregnancy rate |
4.1% |
3.8% |
Table 7. Health Indicators, Bonteheuwel
NETREG clinic, Bonteheuwel |
||
Health indicators |
||
Infant Mortality rate |
2001/02 |
2002/03 |
(per 1000 live births) |
20 |
37.04 |
Teen Pregnancy rate |
7.8% |
6.0% |
III. PURPOSE OF THE ASSESSMENT
This assessment addresses four research questions:
This research process began with the goal of identifying a specific issue area for in-depth assessment to supplement the broad situational analysis already completed in Langa and Bonteheuwel. Through informal interviews focused on general perceptions of health, it was observed that substance abuse and domestic violence were mentioned with significant frequency as two of the biggest health problems in both communities.
Although it was recognized that social issues such as substance abuse and domestic violence might be outside the scope of a normal health needs assessment, the emphasis placed by interview participants on socioeconomic problems required a broad definition of community health. These two issues were particularly intriguing because of their perceived roles as intermediaries on a scale of health issues; for example, an underlying problem of unemployment might lead to substance abuse, which in turn could manifest itself in higher vulnerability to HIV/AIDS.
After selecting these issue areas, subsequent, more focused interviews suggested an emphasis on resource availability and utilization. Several service providers who participated in interviews were working on the same issue without knowing of each other’s existence, while ordinary community members were often unaware of the resources available to them. Identifying opportunities to connect existing resources to each other and their potential clients quickly emerged as an important goal of this assessment.
Finally, the philosophy of community-based participatory research behind the project led to the inclusion of the last question. It was determined that in order to make meaningful recommendations about future programs and research, the incorporation of community voices was necessary. This question also resulted in many of the most interesting and uniquely informative anecdotal responses.